

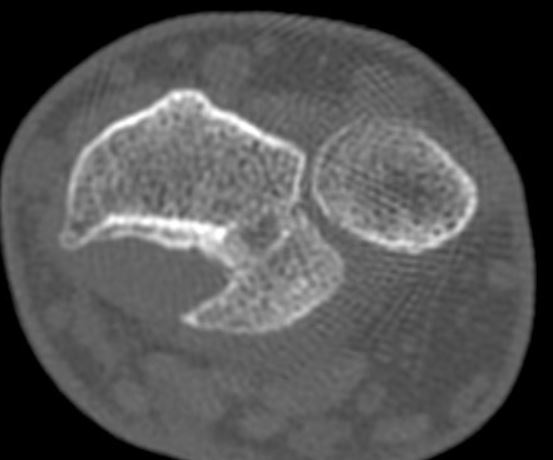
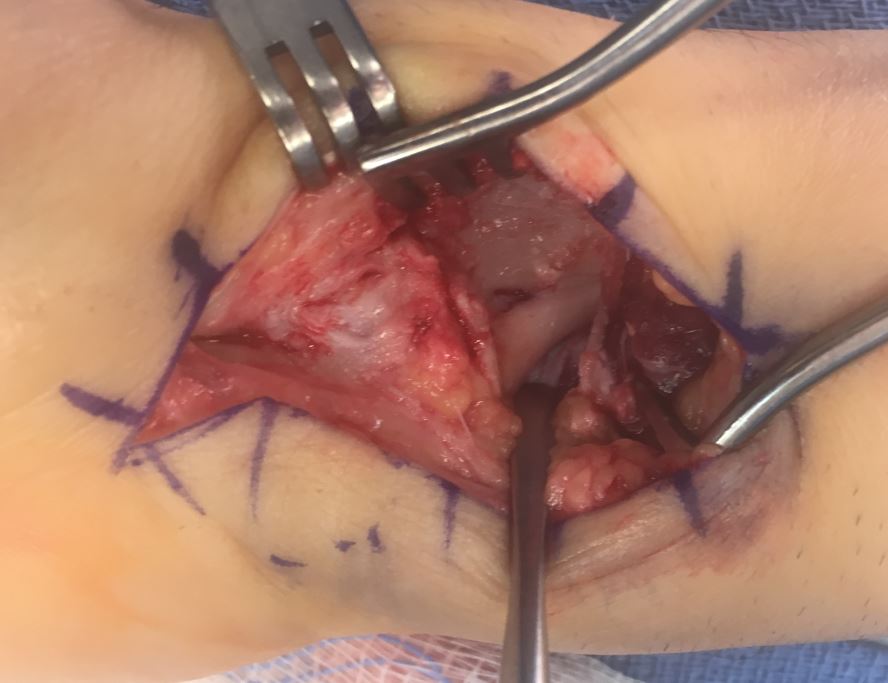
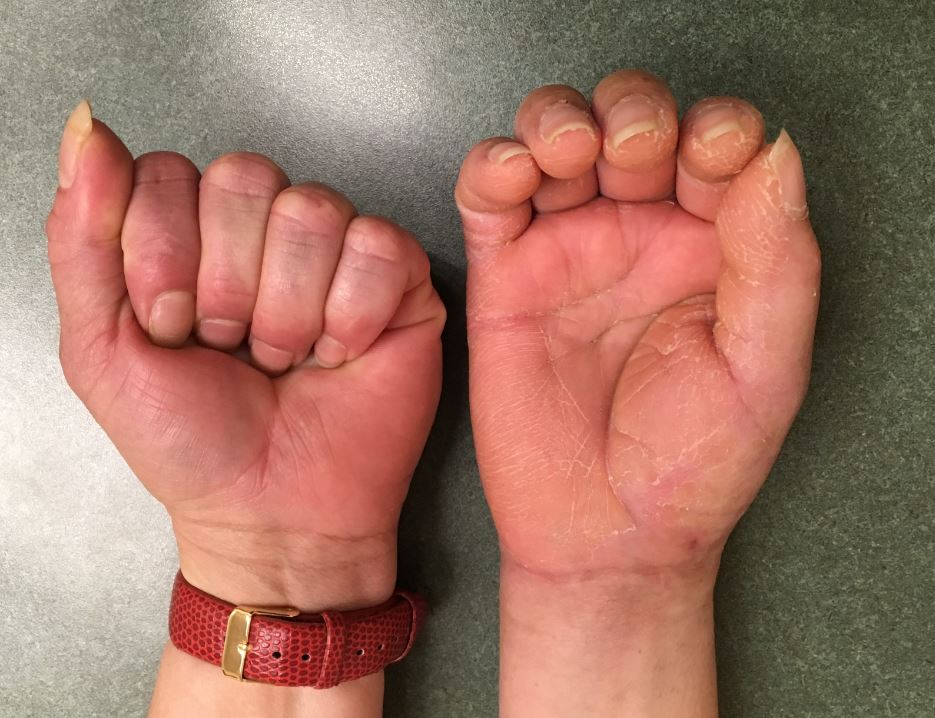
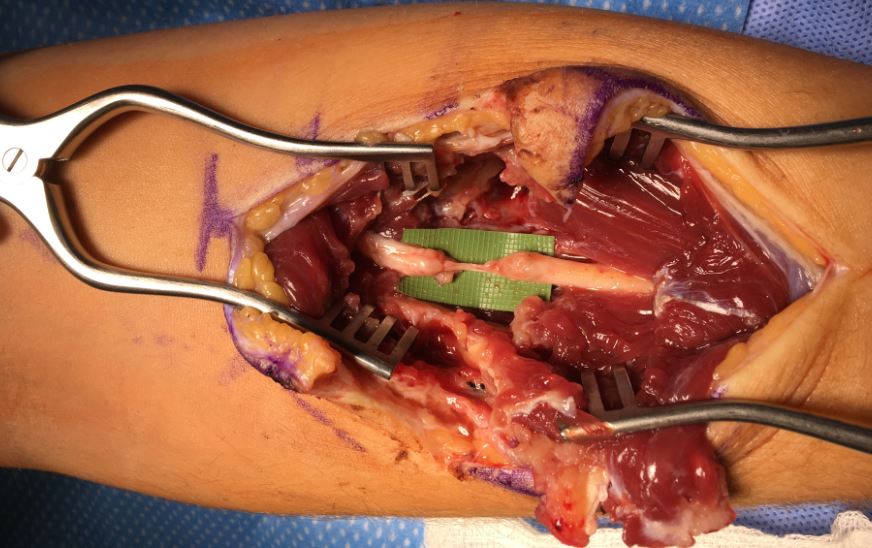
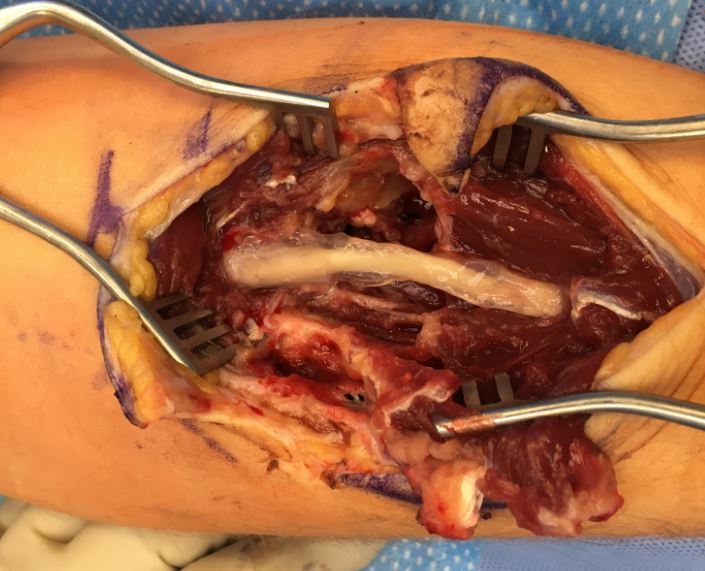
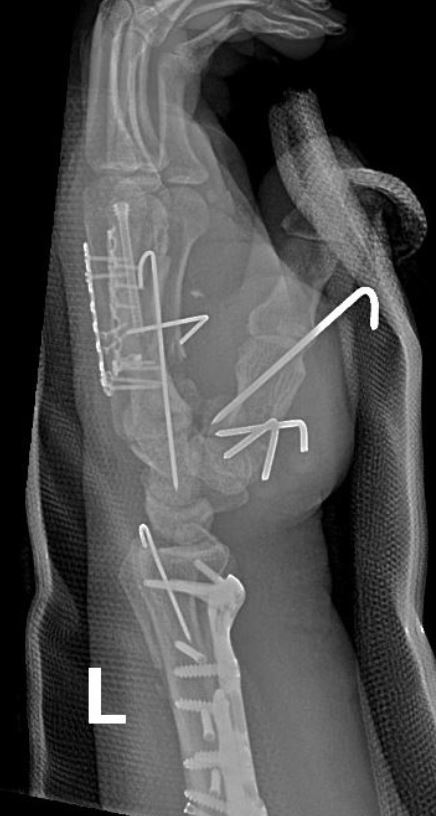
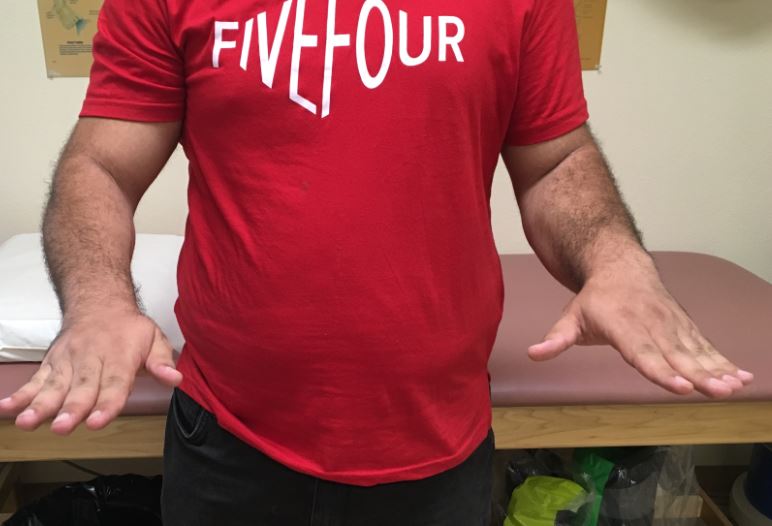
Case Presentation: A 36 year old gentleman sustained a wrist injury while running and falling but xrays at the time were reportedly negative for a fracture. He was given a splint but had continued and persistent pain and swelling. He came to my office 6 months later and xrays and a CT scan showed a dislocated wrist with a malunited lunate facet fragment. Based on his young age and long term function, I recommended an osteotomy to correct the bone and restore the articular surface. The fracture healed uneventfully and he worked aggressively with therapy to regain motion which plateaued at 1 year with wrist flex/ext of 25/55 degrees and supination/pronation of 50/80 degrees.




































































{kind=link}
{kind=link}